Fill Your Medication Administration Record Sheet Form
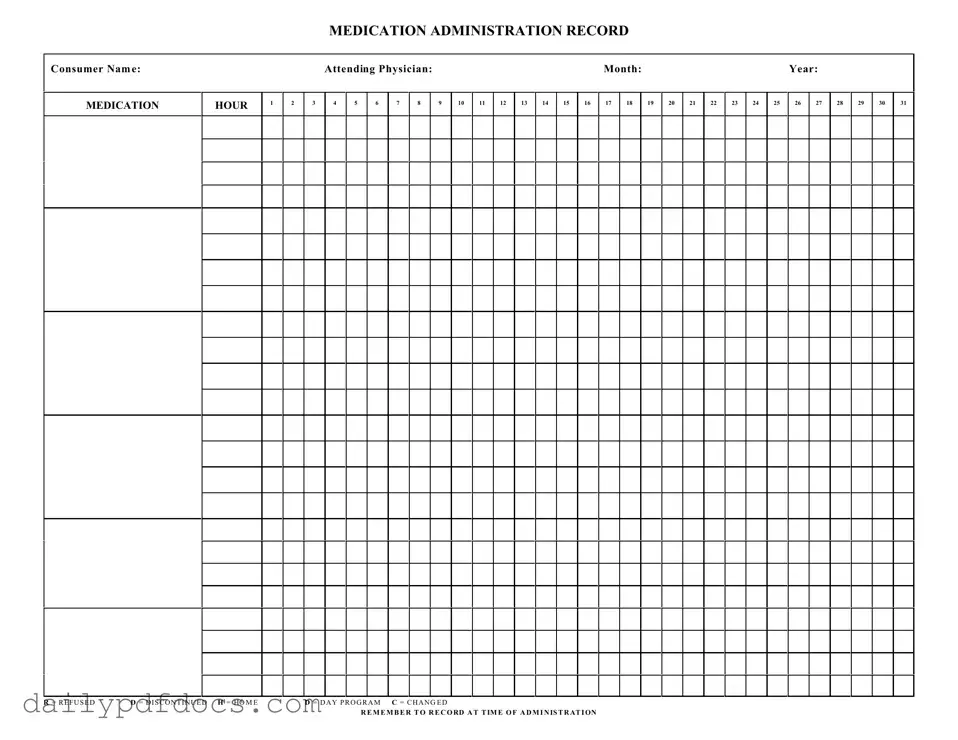
The Medication Administration Record Sheet, often referred to as the MAR sheet, serves as a crucial tool in the healthcare setting, particularly for managing patient medications. This form is designed to ensure accurate documentation of medication administration, which is essential for patient safety and effective treatment. It includes key sections such as the consumer's name and details about the attending physician, allowing for easy identification and accountability. The form is organized by month and year, providing a clear timeline for medication administration. Each day of the month is represented with spaces to record medication doses at specific hours, facilitating precise tracking of when each medication is given. Additionally, it incorporates codes to indicate whether a medication was refused, discontinued, or changed, which helps healthcare providers make informed decisions about ongoing treatment. By recording administration times and any deviations from the prescribed regimen, the MAR sheet promotes a systematic approach to medication management, ultimately enhancing patient care and outcomes.
Find Other Documents
Ms Word Chart - Date: Use a consistent format if multiple entries are being created.
How to Check How Many College Credits You Have - The form is designed to be straightforward for all students.
The Washington Bill of Sale is a legal document that serves as proof of the transfer of ownership for personal property from one party to another. This form is essential for ensuring that both the buyer and seller have a clear record of the transaction, protecting their rights and interests. For those looking to create or obtain this document, you can find useful resources at Washington Templates, ensuring a smooth transfer process.
Employee Change Form Template - Fill out this form to update an employee’s contact information.
Common Questions
What is a Medication Administration Record Sheet?
The Medication Administration Record Sheet is a document used to track the administration of medications to individuals. It helps ensure that medications are given at the correct times and in the appropriate dosages. This record is essential for maintaining accurate medical histories and for communicating with healthcare providers.
Who should use the Medication Administration Record Sheet?
This form is typically used by caregivers, healthcare professionals, and family members responsible for administering medications to individuals. It is particularly important in settings such as group homes, assisted living facilities, and day programs where multiple medications may be given to various consumers.
What information is required on the form?
Essential information includes the consumer's name, the attending physician's name, the month and year of administration, and a detailed schedule for medication administration. Each hour of the day is listed, allowing caregivers to mark when medications are given or if they were refused or discontinued.
How should medications be recorded on the sheet?
When administering medication, caregivers should record the time of administration directly on the form. If a medication is refused, discontinued, or changed, caregivers should use the designated codes (R for Refused, D for Discontinued, and C for Changed) to indicate these actions. This ensures accurate documentation of medication management.
Why is it important to keep this record up to date?
Keeping the Medication Administration Record Sheet up to date is crucial for several reasons. It provides a clear history of what medications have been administered, helps prevent medication errors, and ensures that healthcare providers have accurate information for making treatment decisions. Regular updates also assist in monitoring the consumer's response to medications.
What should be done if a mistake is made on the form?
If a mistake occurs on the Medication Administration Record Sheet, it is important to correct it promptly. Cross out the incorrect entry with a single line, and initial the correction to indicate who made the change. This maintains a clear record while showing that an error was acknowledged and corrected.
Where can I find additional resources or support regarding this form?
Additional resources regarding the Medication Administration Record Sheet can often be found through healthcare providers, local health departments, or online medical resources. Caregivers may also seek guidance from training programs focused on medication management and administration.
Preview - Medication Administration Record Sheet Form
MEDICATION ADMINISTRATION RECORD
Consumer Nam e:
MEDICATION
HOUR
1
2
|
Attending Physician: |
|
|
|
|
|
|
|
|
Month: |
|
|
|
|
|
|
|
Year: |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
4 |
5 |
6 |
7 |
8 |
|
9 |
10 |
11 |
12 |
13 |
14 |
15 |
16 |
17 |
18 |
|
19 |
20 |
21 |
22 |
23 |
24 |
25 |
26 |
27 |
28 |
29 |
30 |
31 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R = R E F U S E D |
D = D I S C O N T I N U E D H = HO M E |
D = D A Y P R O G R A M C = C H A N G E D |
R E M E M B E R T O R E C O RD A T T IM E O F A D M I N IS T R AT I ON
Similar forms
The Medication Administration Record Sheet is similar to several other documents used in healthcare settings. Each document serves a specific purpose but shares common elements in tracking and documenting patient care. Here are nine similar documents:
- Patient Care Record: This document records all aspects of a patient's care, including medications, treatments, and observations, similar to how the Medication Administration Record tracks medication administration.
- Last Will and Testament Form: For those preparing their estate, the step-by-step Last Will and Testament guide provides essential legal documentation for outlining asset distribution and wishes.
- Medication Reconciliation Form: Used to ensure that a patient's medication list is accurate and complete, this form shares the goal of preventing medication errors, just like the Medication Administration Record.
- Vital Signs Record: This document tracks a patient's vital signs over time. Both records help healthcare providers monitor patient health and make informed decisions.
- Nursing Notes: Nurses document patient observations and care provided. This document complements the Medication Administration Record by providing context for medication administration.
- Incident Report: Used to document any unexpected events affecting patient safety, this report is similar in that it requires accurate and timely documentation, much like the Medication Administration Record.
- Treatment Plan: This outlines the specific treatments a patient will receive. It connects to the Medication Administration Record by detailing the medications included in the treatment.
- Discharge Summary: This document summarizes a patient’s hospital stay and includes medication instructions. It shares the purpose of ensuring continuity of care, similar to the Medication Administration Record.
- Clinical Pathway: This outlines the expected course of treatment for a specific condition. It includes medication administration schedules, aligning closely with the Medication Administration Record.
- Progress Notes: These are written by healthcare providers to document a patient's progress. They provide context for medication administration, similar to the information captured in the Medication Administration Record.
Misconceptions
Understanding the Medication Administration Record Sheet (MARS) is crucial for anyone involved in healthcare. However, several misconceptions can lead to confusion. Here are five common misunderstandings:
- It's only for nurses to use. Many people think that only registered nurses can fill out the MARS. In reality, anyone administering medication, including caregivers and aides, should be familiar with it to ensure proper documentation.
- It’s optional to record refusals or changes. Some believe that documenting when a patient refuses medication or when a medication is changed is not necessary. This is incorrect. Accurate records help in tracking patient care and ensuring safety.
- All medications are listed on the MARS. Many assume that every medication a patient takes will automatically appear on the MARS. However, it’s essential to verify that all prescribed medications are documented. Missing entries can lead to serious errors.
- Only the physician can make changes to the MARS. Some think that only physicians have the authority to update the record. In truth, any qualified healthcare provider can make necessary changes, but they must follow proper protocols and communicate with the team.
- Recording is only needed at the end of the day. There’s a misconception that it’s sufficient to fill out the MARS at the end of a shift. In fact, recording should happen at the time of administration to ensure accuracy and accountability.
Clearing up these misconceptions can enhance the safety and effectiveness of medication administration. Understanding how to properly use the MARS is a vital part of patient care.
File Attributes
| Fact Name | Description |
|---|---|
| Purpose | The Medication Administration Record (MAR) is used to document the administration of medications to consumers in various settings, ensuring proper tracking and accountability. |
| Consumer Information | Each MAR includes essential consumer details, such as the consumer's name and the attending physician's name, to maintain clarity and accuracy. |
| Monthly Tracking | The MAR is organized by month and year, allowing caregivers to track medication administration daily throughout the month. |
| Administration Hours | The form provides designated hours for medication administration, helping ensure that medications are given at the correct times. |
| Medication Status Codes | Codes such as R (Refused), D (Discontinued), H (Home), D (Day Program), and C (Changed) are used to indicate the status of each medication entry. |
| Legal Compliance | In many states, the use of a MAR is governed by specific healthcare regulations, which mandate accurate record-keeping for patient safety. |
| Documentation Requirement | It is crucial to record the administration of medications at the time they are given, ensuring that the records reflect real-time information. |
| Importance of Accuracy | Accurate completion of the MAR is vital for preventing medication errors and ensuring that consumers receive their prescribed treatments safely. |