Fill Your DD 2870 Form
The DD 2870 form is an essential document for individuals seeking to access their medical records and other health-related information from the Department of Defense (DoD). This form serves as a request for the release of personal health information, ensuring that service members, veterans, and their families can obtain the medical records necessary for their care and well-being. It is crucial to understand that the DD 2870 not only facilitates the transfer of medical data but also establishes the legal framework for the privacy and confidentiality of that information. By completing this form, individuals assert their rights to access their health records, which can be vital for ongoing medical treatment, disability claims, or personal health management. Additionally, the form includes sections that allow for the specification of the type of information requested, as well as the intended purpose for which it will be used. Timeliness is key, as delays in obtaining these records can impede necessary medical decisions. Therefore, understanding how to properly fill out and submit the DD 2870 is of utmost importance for anyone navigating the complexities of military healthcare and seeking to ensure their rights are upheld.
Find Other Documents
Intent to Lien Letter Template Free - This document ensures compliance with Florida’s laws regarding liens and payments.
How to Terminate Parental Rights in Sc - Each section of the form has a purpose, contributing to the overall clarity of the relinquishment.
The Washington Articles of Incorporation form is a legal document that establishes a corporation in the state of Washington. This form outlines essential details about the corporation, such as its name, purpose, and registered agent. For more guidance on completing the necessary documentation, you can refer to the resources provided by Washington Templates, which can help ensure you meet all requirements. Completing this form is a crucial step in starting your business, so be sure to fill it out by clicking the button below.
Miscarriage Paperwork From Doctor - It provides an avenue for further action if families wish to pursue registration.
Common Questions
What is the DD 2870 form?
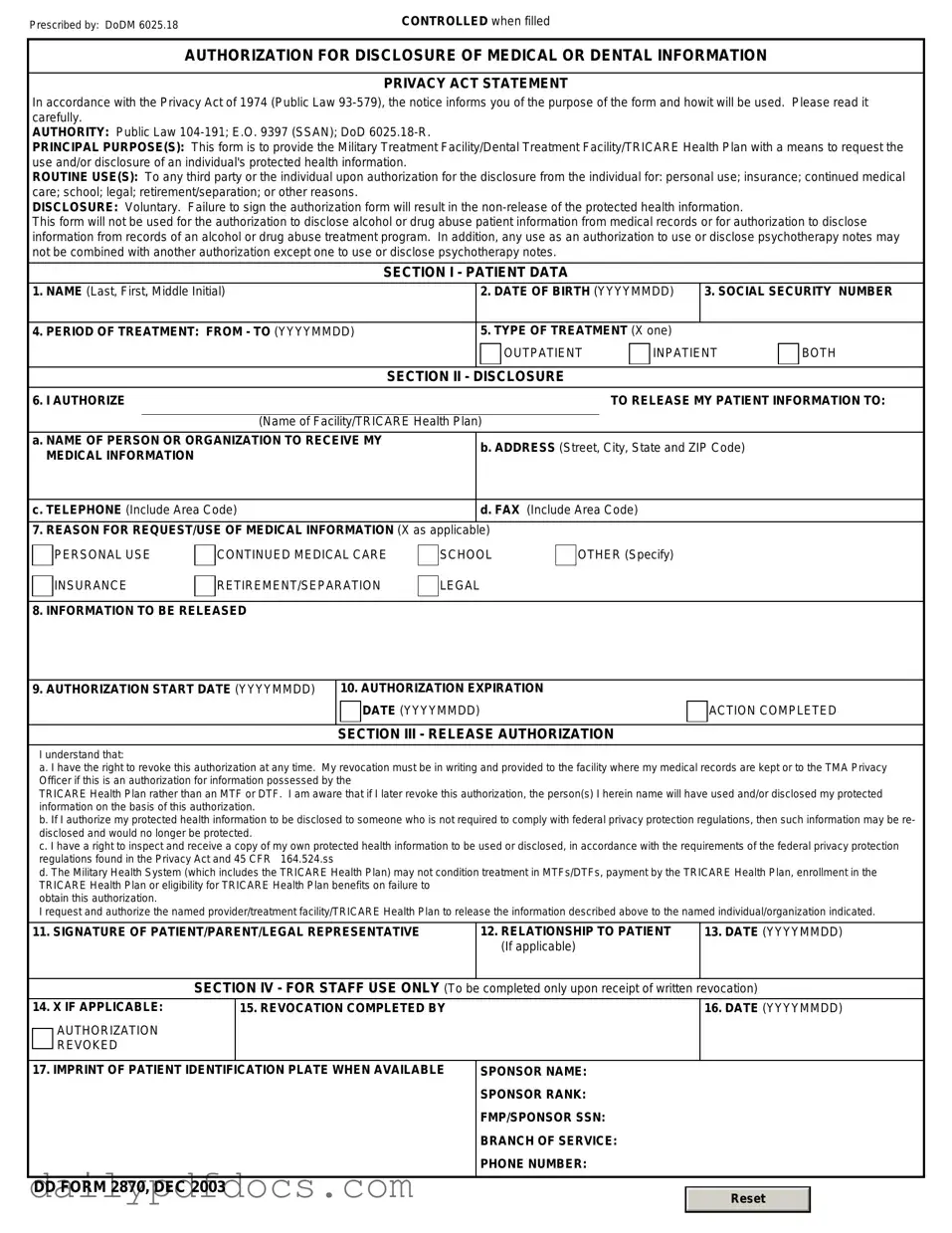
The DD 2870 form, also known as the "Authorization for Disclosure of Medical or Dental Information," is a document used by military personnel and their dependents. It allows individuals to authorize the release of their medical or dental information to specified parties. This is crucial for ensuring that healthcare providers can access necessary records for treatment, referrals, or insurance purposes.
Who needs to fill out the DD 2870 form?
Any active duty service member, reservist, or dependent who requires their medical or dental records to be shared with another party should complete the DD 2870 form. This includes situations such as transferring care to a new provider, seeking treatment outside the military healthcare system, or when required for insurance claims.
How do I obtain a DD 2870 form?
You can obtain the DD 2870 form from various sources. It is available online through the official Department of Defense website or military health system portals. Additionally, you can request a hard copy from your healthcare provider or military medical facility. Make sure to use the most recent version of the form to avoid any issues.
What information do I need to provide on the DD 2870 form?
When filling out the DD 2870 form, you will need to provide personal information such as your name, Social Security number, and contact details. You must also specify the type of medical or dental information you wish to disclose and the parties to whom the information will be released. Be clear and detailed to ensure the request is processed smoothly.
Is there a deadline for submitting the DD 2870 form?
There is no specific deadline for submitting the DD 2870 form. However, it is advisable to submit it as soon as you know that you need your medical or dental records shared. Delays in submitting the form could impact your ability to receive timely care or process insurance claims.
Can I revoke the authorization given in the DD 2870 form?
Yes, you can revoke the authorization at any time. To do so, you should submit a written request to the same parties to whom you authorized the disclosure. This revocation will prevent any further release of your medical or dental information after the date of your request.
What happens if I do not fill out the DD 2870 form?
If you do not complete the DD 2870 form when needed, your healthcare provider may not be able to access your medical or dental records. This could lead to delays in treatment, miscommunication about your health status, or complications with insurance claims. Therefore, it is important to fill out the form whenever necessary.
Preview - DD 2870 Form
Prescribed by: DoDM 6025.18 |
CONTROLLED when filled |
AUTHORIZATION FOR DISCLOSURE OF MEDICAL OR DENTAL INFORMATION
PRIVACY ACT STATEMENT
In accordance with the Privacy Act of 1974 (Public Law
AUTHORITY: Public Law
PRINCIPAL PURPOSE(S): This form is to provide the Military Treatment Facility/Dental Treatment Facility/TRICARE Health Plan with a means to request the use and/or disclosure of an individual's protected health information.
ROUTINE USE(S): To any third party or the individual upon authorization for the disclosure from the individual for: personal use; insurance; continued medical care; school; legal; retirement/separation; or other reasons.
DISCLOSURE: Voluntary. Failure to sign the authorization form will result in the
This form will not be used for the authorization to disclose alcohol or drug abuse patient information from medical records or for authorization to disclose information from records of an alcohol or drug abuse treatment program. In addition, any use as an authorization to use or disclose psychotherapy notes may not be combined with another authorization except one to use or disclose psychotherapy notes.
SECTION I - PATIENT DATA
1. NAME (Last, First, Middle Initial) |
|
2. DATE OF BIRTH (YYYYMMDD) |
3. SOCIAL SECURITY NUMBER |
|||
|
|
|
|
|
|
|
4. PERIOD OF TREATMENT: FROM - TO (YYYYMMDD) |
|
5. TYPE OF TREATMENT (X one) |
|
|
||
|
|
|
OUTPATIENT |
INPATIENT |
BOTH |
|
|
|
|
|
|
|
|
|
|
SECTION II - |
DISCLOSURE |
|
|
|
6. I AUTHORIZE |
|
|
TO RELEASE MY PATIENT INFORMATION TO: |
|||
|
|
|
|
|
||
|
(Name of Facility/TRICARE Health Plan) |
|
|
|
||
a. NAME OF PERSON OR ORGANIZATION TO RECEIVE MY |
|
b. ADDRESS (Street, City, State and ZIP Code) |
|
|||
MEDICAL INFORMATION |
|
|
||||
|
|
|
|
|
||
|
|
|
|
|
||
c. TELEPHONE (Include Area Code) |
|
d. FAX (Include Area Code) |
|
|
||
|
|
|
|
|
||
7. REASON FOR REQUEST/USE OF MEDICAL INFORMATION (X as applicable) |
|
|
|
|
||
PERSONAL USE
INSURANCE
CONTINUED MEDICAL CARE
RETIREMENT/SEPARATION
SCHOOL
LEGAL
OTHER (Specify)
8. INFORMATION TO BE RELEASED
9. AUTHORIZATION START DATE (YYYYMMDD)
10. AUTHORIZATION EXPIRATION
DATE (YYYYMMDD)
SECTION III - RELEASE AUTHORIZATION
ACTION COMPLETED
I understand that:
a. I have the right to revoke this authorization at any time. My revocation must be in writing and provided to the facility where my medical records are kept or to the TMA Privacy Officer if this is an authorization for information possessed by the
TRICARE Health Plan rather than an MTF or DTF. I am aware that if I later revoke this authorization, the person(s) I herein name will have used and/or disclosed my protected information on the basis of this authorization.
b. If I authorize my protected health information to be disclosed to someone who is not required to comply with federal privacy protection regulations, then such information may be re- disclosed and would no longer be protected.
c. I have a right to inspect and receive a copy of my own protected health information to be used or disclosed, in accordance with the requirements of the federal privacy protection regulations found in the Privacy Act and 45 CFR 164.524.ss
d. The Military Health System (which includes the TRICARE Health Plan) may not condition treatment in MTFs/DTFs, payment by the TRICARE Health Plan, enrollment in the TRICARE Health Plan or eligibility for TRICARE Health Plan benefits on failure to
obtain this authorization.
I request and authorize the named provider/treatment facility/TRICARE Health Plan to release the information described above to the named individual/organization indicated.
11. SIGNATURE OF PATIENT/PARENT/LEGAL REPRESENTATIVE |
12. RELATIONSHIP TO PATIENT |
13. DATE (YYYYMMDD) |
|
(If applicable) |
|
|
|
|
SECTION IV - FOR STAFF USE ONLY (To be |
completed only upon receipt of written revocation) |
|
14. X IF APPLICABLE:
AUTHORIZATION REVOKED
15. REVOCATION COMPLETED BY
16.DATE (YYYYMMDD)
17. IMPRINT OF PATIENT IDENTIFICATION PLATE WHEN AVAILABLE |
SPONSOR NAME: |
||
|
SPONSOR RANK: |
||
|
FMP/SPONSOR SSN: |
||
|
BRANCH OF SERVICE: |
||
|
PHONE NUMBER: |
||
|
|
|
|
DD FORM 2870, DEC 2003 |
|
|
|
|
Reset |
|
|
|
|
|
|
|
|
|
|
Similar forms
The DD 2870 form is a document used by the U.S. Department of Defense for requesting medical care and services. Several other forms serve similar purposes in different contexts. Here are seven documents that are comparable to the DD 2870:
- VA Form 10-10EZ: This form is used by veterans to apply for health benefits through the Department of Veterans Affairs. Like the DD 2870, it collects personal information to determine eligibility for medical services.
- Missouri Mobile Home Bill of Sale: This legal document is essential for transferring ownership of a mobile home and includes key details about the transaction. For more information, visit mobilehomebillofsale.com/blank-missouri-mobile-home-bill-of-sale.
- CMS-1500: This is a standard claim form used by healthcare providers to bill Medicare and other insurers. It includes patient information and details about the services provided, similar to the information collected on the DD 2870.
- SF-180: The Standard Form 180 is used to request military records. It shares the purpose of gathering essential information from individuals to facilitate access to services or records, akin to the DD 2870.
- Form 21-526EZ: This is a claim for disability compensation and related compensation benefits for veterans. It requires personal details and medical information, paralleling the data collection in the DD 2870.
- Form 1040: While primarily a tax form, the IRS Form 1040 includes personal and financial information that may be relevant for healthcare-related tax deductions, similar to the personal data collected in the DD 2870.
- Form I-485: This is used to apply for a green card in the United States. It collects personal and medical information, much like the DD 2870, to assess eligibility for benefits.
- Form W-2: This form reports an employee's annual wages and taxes withheld. It is similar in that it provides essential personal information that may be relevant for healthcare benefits and services.
Misconceptions
The DD 2870 form is an important document used in military and veteran contexts, yet many misconceptions surround it. Understanding these misconceptions can help individuals navigate the process more effectively. Below is a list of common misunderstandings regarding the DD 2870 form.
- It is only for active duty service members. Many believe that the DD 2870 form is exclusively for active duty personnel. In reality, it is also applicable to veterans and certain family members.
- It is a complicated form. Some think that the DD 2870 form is overly complex. While it may seem intimidating at first, the form is straightforward and can be completed with careful attention to the instructions.
- Submission is optional. There is a misconception that submitting the DD 2870 is not mandatory. However, for those seeking specific benefits, timely submission of this form is often essential.
- It only applies to health benefits. Many individuals assume the DD 2870 form is limited to health care services. In fact, it can also be relevant for other benefits, such as educational assistance.
- All information is public. Some believe that the information provided on the DD 2870 is accessible to the public. However, personal information is kept confidential and protected.
- It can be submitted at any time. A common misconception is that there are no deadlines for submitting the DD 2870. In truth, there are specific timeframes that must be adhered to, depending on the benefits being sought.
- It is only for those with prior claims. Many think the DD 2870 form is only necessary for individuals who have previously filed claims. New applicants also need to complete this form to initiate their requests.
- Help is not available. Some feel that they must navigate the form alone. However, assistance is often available through various military and veteran organizations, making the process more manageable.
- Filling it out incorrectly is not a big deal. There is a belief that minor mistakes on the DD 2870 form won’t matter. Unfortunately, errors can lead to delays or even denials of benefits.
- Once submitted, it cannot be changed. Some people think that after the DD 2870 is submitted, no changes can be made. In fact, if you realize a mistake, it is possible to submit a corrected form.
By addressing these misconceptions, individuals can approach the DD 2870 form with greater confidence and clarity. Understanding the purpose and requirements of this document is crucial for accessing the benefits available to military personnel and veterans.
File Attributes
| Fact Name | Description |
|---|---|
| Purpose | The DD Form 2870 is used to request medical records or information from the Department of Defense. |
| Eligibility | Active duty service members, veterans, and their authorized representatives can use this form. |
| Privacy Act Compliance | This form is compliant with the Privacy Act of 1974, ensuring that personal information is protected. |
| Submission Process | The completed form must be submitted to the appropriate military medical facility or records office. |
| State-Specific Forms | Some states may have their own forms for medical record requests, governed by state health privacy laws. |
| Information Required | Users must provide personal identification details, such as name, Social Security number, and date of birth. |
| Processing Time | Processing times for requests can vary, but typically take several weeks to complete. |
| Cost | There is usually no fee for obtaining records through this form for eligible individuals. |
| Record Types | The form can be used to request various types of medical records, including outpatient and inpatient records. |
| Contact Information | For questions, individuals can contact the records office directly, often listed on the form or military facility website. |